Research funded by: NHMRC Partnership Centre for Dealing with Cognitive and Related Functional Decline in Older People
The AD-5D is a preference-based scoring algorithm that derives utility weights for people with dementia from the QOL-AD (Quality of Life – Alzheimer’s Disease), a widely-used instrument for measuring quality of life for people with dementia.
The AD-5D was developed by eliciting values for a selection of health states and conducting statistical modelling to develop an algorithm that derives utility values for all possible health states defined by the AD-5D descriptive system (summarised in Figure 1). This algorithm enables data collected from any administration of the QOL-AD to be used in the economic evaluation of treatments and interventions for people diagnosed with dementia – both prospective and retrospective studies.
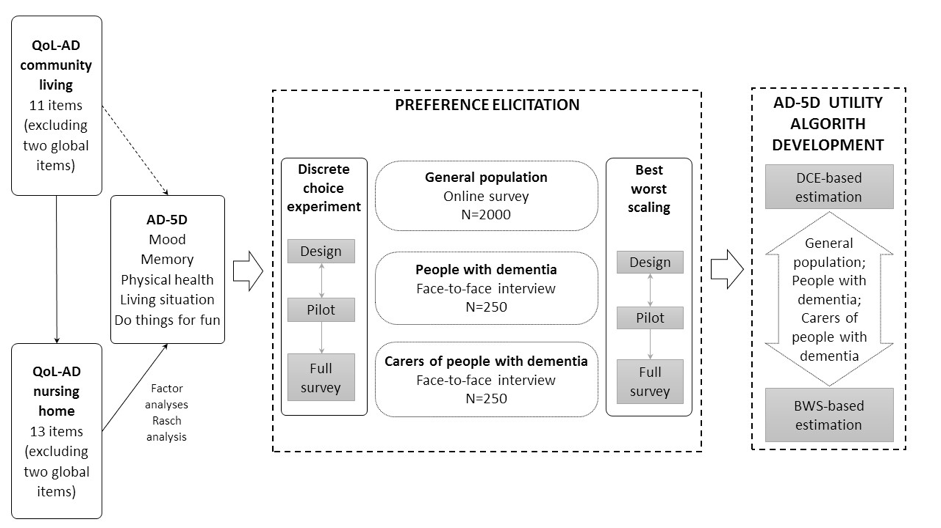
Establishing the dimensions
Exploratory and confirmatory factor analyses were conducted using data collected from 284 residents living in long-term care facilities in Australia who had a diagnosis of dementia and had completed 13 items of the QOL-AD nursing home version (excluding two general health items). Further assessment of the structure of the measure was conducted to ensure coverage of the key areas of quality of life. Rasch analysis was then used to test the psychometric performance of the items, and select item(s) to describe each dimension.
Preference elicitation: general population
A web-based survey was administered to a sample of 2000 members of the Australian general population in October to December 2017. In addition to instructional information and demographic data collection, participants completed Discrete Choice Experiment with time trade-off (DCETTO) (ten choice sets) and Best Worst Scaling (BWS) (four choice sets) tasks. The order of tasks was randomly assigned to eliminate order effects bias in the responses.
Preference elicitation: people with dementia and their carers
A web-based survey was administered to 84 dementia dyads (people living with dementia and a family carer) via interview. The survey included a simple cognition test for the person with dementia (the GP-Cog). Demographic information was collected along with information about the current health-related quality of life of both the person with dementia and their carer, using the Quality of Life – Alzheimer’s disease (QOL-AD) (self- and proxy-rated by the carer) and the EQ-5D. DCETTO and BWS were completed by the person with dementia and proxy-rated by the carer.
Validation studies
Content validity of the AD-5D dimensions was assessed using the Q methodology. Three focus groups (Brisbane, Sydney and Adelaide) were conducted with people with dementia, carers for people with dementia, and general community members. Analysis of focus group transcripts and outputs demonstrated that all activities impacting quality of life for people with dementia could be mapped to one of the five AD-5D domains: memory, mood, physical health, living situation, and do things for fun. The domains considered most important for quality of life differed between people with dementia, their caregivers and members of the community, with memory the least important domain for all three groups. The rationale for priorities also varied between groups.